A broken bone is supposed to be a temporary problem. The fracture is treated, the bone heals, and life goes back to normal. But for some patients the story does not end there. Months after the injury, the pain is still present. The limb looks bent or shorter than before. Walking, lifting, or even standing feels unstable. In some cases, a surgery done earlier has failed, and the patient is left wondering whether anything can still be done.
The answer, in most cases, is yes. Fractures that have failed to heal (non-union) or healed in the wrong position (malunion) can very often be corrected, even years after the original injury. Modern reconstruction techniques such as revision fixation, bone grafting, corrective osteotomy, and ring fixators can restore alignment, strength, and mobility.
Every year, thousands of international patients, including many from Africa and the Middle East, travel to India for this kind of advanced orthopedic care. The reasons are practical: highly experienced trauma and reconstruction surgeons, modern imaging and surgical planning, structured rehabilitation, short waiting times, and costs that are a fraction of those in Western countries. This guide explains what non-union and malunion mean, how they are treated, what the treatment costs in India, and how to get your case reviewed from home.
When to seek urgent care: If the area around an old fracture or previous surgery becomes red, warm, or swollen, if there is pus or discharge from the wound or an old scar, or if you develop fever with increasing pain, see a doctor promptly. These can be signs of bone infection (osteomyelitis), which needs early treatment and can worsen quickly if ignored.
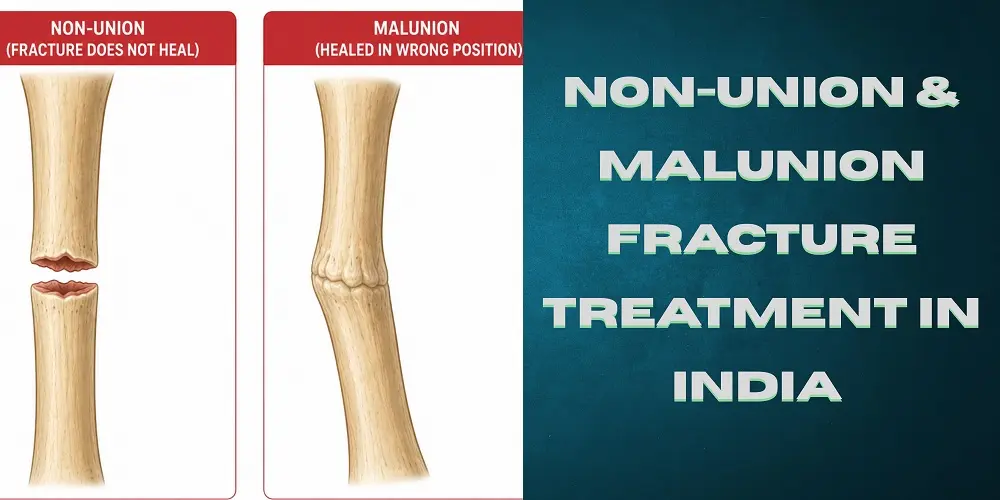
What Are Non-Union and Malunion Fractures?
Bone is living tissue, and under the right conditions it repairs itself after a fracture. Healing, however, needs three things: a good blood supply, stability at the fracture site, and time. When any of these is missing, healing goes wrong in one of two ways.
Non-union: The bone fails to heal at all. The two ends of the fracture remain separate, and the gap fills with scar tissue instead of solid bone. The area stays painful and often feels loose or unstable. Doctors generally diagnose non-union when a fracture shows no signs of healing for several months (commonly 6 to 9 months after injury, or when there has been no visible progress on X-rays for 3 consecutive months).
Malunion: The bone does heal, but in the wrong position. It may be bent (angulated), twisted (rotated), overlapped, or shortened. The result can be a visible deformity, a limp, uneven limb length, pain in nearby joints that are forced to work at the wrong angle, and early arthritis if a joint surface is involved.
There is also a middle category called delayed union, where the bone is healing but much more slowly than expected. Delayed union sometimes recovers with conservative care, but it needs close monitoring because it can progress to full non-union.
The key message for patients: neither condition means the bone can never heal. It means the healing process needs help, and that help is a well-established part of modern orthopedic surgery.
Common Causes of Non-Union and Malunion
Failed healing is rarely the patient's fault. It usually comes down to the severity of the original injury, the quality of the initial treatment, or medical factors that slow bone repair:
- Severe trauma: High-energy injuries from road accidents or falls from height damage not just the bone but also the surrounding muscle and blood vessels that the bone needs for healing
- Open (compound) fractures: When the bone breaks through the skin, the risk of contamination and infection rises sharply, and infection is one of the strongest blockers of bone healing
- Delayed or missed treatment: Fractures that were never properly aligned and immobilized, often because treatment was unavailable, unaffordable, or delayed, frequently heal in the wrong position or not at all. This is one of the most common situations we see in patients from regions with limited trauma care
- Bone infection: Infection at the fracture site (osteomyelitis) destroys healing tissue and must be controlled before the bone can be reconstructed
- Poor fixation or failed previous surgery: Plates, screws, or rods that were too weak, wrongly positioned, or that loosened over time leave the fracture unstable, and an unstable fracture cannot heal
- Bone loss after injury: When a piece of bone is missing after a severe injury, the gap may be too large for the body to bridge on its own
- Health and lifestyle factors: Smoking, diabetes, poor nutrition, vitamin D deficiency, anemia, and some medicines all slow down bone repair
Signs That You May Need Fracture Reconstruction
Consider a specialist review if you notice any of the following, whether your injury was recent or years ago:
- Pain at the fracture site that continues months after the injury or previous surgery
- A feeling of movement, looseness, or instability at the old fracture
- A visible bend, twist, or bump in the limb
- One arm or leg noticeably shorter than the other, or a new limp
- Difficulty bearing weight, gripping, or using the limb normally
- Movement of nearby joints becoming limited or painful
- X-rays that show the fracture line still visible many months later
- A previous fixation surgery where the implant has loosened, bent, or broken
None of these signs mean it is too late. Even old, neglected fractures and failed surgeries can usually be reconstructed. The sooner the evaluation happens, though, the simpler the treatment tends to be.
How Doctors Confirm the Diagnosis
The good news for international patients: the tests needed to plan treatment are simple, and most of them may already be in your file.
- X-rays: Standard X-rays from at least two angles show whether the fracture line is still open, how the bone ends are positioned, and the state of any implants
- CT scan: A CT scan gives a three-dimensional picture of the fracture gap and is the most reliable way to confirm non-union and to plan corrective surgery
- Blood tests: Blood tests such as CBC, ESR, and CRP help detect hidden infection, and vitamin D and calcium levels identify healing problems that should be corrected
- Infection work-up: If infection is suspected, an MRI or a bone scan may be added, and occasionally a sample is taken to identify the bacteria before planning staged surgery
If you already have recent X-rays or a CT scan, surgeons can review them remotely and give a provisional treatment plan and cost estimate before you travel. Any missing tests can be completed within a day or two at the treating hospital in India.
Treatment Options in India
There is no single operation for failed fracture healing. The right procedure depends on which bone is involved, whether the problem is non-union or malunion, whether infection is present, and how much bone quality remains. These are the approaches used at major Indian orthopedic centres:
Revision fixation
The old, failed implant is removed and the fracture is freshly stabilized with new plates, rods (nails), or screws, restoring the stability the bone needs to heal. This is often combined with bone grafting.
Bone grafting
Healthy bone, usually taken from the patient's own pelvis, is packed into the fracture gap. The graft acts as a scaffold and a biological stimulus that restarts the healing process. For larger defects, surgeons may use special techniques such as vascularized grafts or synthetic bone substitutes.
Corrective osteotomy
This is the main operation for malunion. The surgeon carefully re-cuts the bone at the site where it healed in the wrong position, realigns it to the correct angle, rotation, and length, and fixes it in the new position. Modern 3D planning from CT scans allows very precise correction.
External fixation and the Ilizarov technique
For infected non-unions, bone loss, or limb shortening, surgeons may use a ring fixator (the Ilizarov method) fitted around the limb from outside. It can hold the bone stable, gradually correct deformity, and even grow new bone to fill gaps and regain length, millimetre by millimetre. Indian centres have decades of experience with this technique and handle some of the most complex reconstruction cases in the world with it.
Infection control before reconstruction
If the fracture site is infected, reconstruction is done in stages: first the infection is cleared with surgical cleaning (debridement), antibiotic beads or spacers, and targeted antibiotics; only then is the final fixation and grafting performed. Skipping this step is a common reason earlier surgeries fail, so a proper staged plan matters.
Joint reconstruction
When the malunion involves a joint surface, such as the hip, knee, ankle, shoulder, or elbow, and the cartilage is badly damaged, the best option may be joint reconstruction or replacement in the same treatment plan.
Recovery and Rehabilitation
Reconstruction is half the treatment; rehabilitation is the other half. A typical journey looks like this:
- Hospital stay: Most patients spend 3 to 7 days in hospital depending on the procedure. Pain is controlled with modern multimodal methods, so patients can start moving early
- Early physiotherapy: Physiotherapy usually begins within a day or two of surgery, first with gentle joint movement and muscle activation, then a structured strengthening program
- Gradual weight bearing: Weight bearing is increased step by step as X-rays confirm the bone is uniting. Depending on the bone and procedure, full weight bearing typically takes 6 to 12 weeks, and complete bone healing 3 to 6 months. Ilizarov treatment for bone loss can take longer
- Follow-up imaging: Follow-up X-rays at regular intervals confirm the correction is holding and the bone is filling in. For international patients, later follow-ups can usually be done from home by sharing X-rays online with the operating surgeon
- What the patient controls: Attending physiotherapy consistently, not smoking, eating enough protein, and correcting vitamin D deficiency measurably improve the chances of solid healing. Compliance is the one part of the outcome that is fully in the patient's hands
International patients usually stay in India for about 2 to 4 weeks in total, depending on the procedure. Before you fly home, the surgical team confirms the fixation is stable, teaches the rehabilitation program, and hands over complete records for your local doctor.
Cost of Non-Union and Malunion Surgery in India
Cost is usually the deciding factor for patients whose first treatment failed, because a second surgery at Western prices is out of reach for many families. India changes that equation:
| Procedure | Approximate Cost in India (USD) |
| Open reduction and internal fixation (ORIF) | $4,000 to $6,000 |
| Revision fixation with bone grafting | $5,000 to $8,000 |
| Corrective osteotomy for malunion | $5,500 to $9,000 |
| Staged reconstruction (infection control + fixation) or Ilizarov / external fixator treatment | $6,000 to $12,000 |
Note: These are indicative package ranges. The exact cost depends on the bone involved, the implant used, whether grafting or staged infection control is needed, and the hospital and city you choose. The same procedures typically cost 5 to 10 times more in the US or Western Europe.
Packages at accredited hospitals generally include the surgeon and anesthesia fees, operating theatre, implants, hospital stay, and in-hospital physiotherapy. You can see the baseline pricing on our ORIF cost in India page. For an exact quote for your case, share your X-rays for a free assessment; reconstruction pricing is always case-specific.
Why International Patients Choose India for Fracture Reconstruction
Experience with complex and neglected cases: Indian trauma centres treat enormous case volumes, which means surgeons who deal with complex non-unions, infected fractures, and neglected injuries every week, not a few times a year
- Advanced technology: 3D CT-based planning, image-guided surgery, modern implants, and dedicated bone banks for grafting
- Accredited hospitals with international support: JCI and NABH accredited hospitals with international patient departments, interpreters, and halal food options
- No waiting lists: Surgery can usually be scheduled within days of your reports being reviewed, not months
- Rehabilitation built into the plan: In-house physiotherapy teams and structured rehab protocols, with remote follow-up after you return home
- Affordability: World-class treatment at a fraction of Western costs, with transparent package pricing before you travel
To choose your team, start with our lists of the best orthopedic surgeons in India, the best orthopedic hospitals in India, and our guide to the top 10 orthopedic hospitals in India.
A fracture that did not heal, or healed in the wrong shape, is not the end of the road. Non-union and malunion are well-understood problems with reliable surgical solutions, from bone grafting and revision fixation to precise corrective osteotomy and Ilizarov reconstruction. What matters is getting the right plan from a team that handles these cases every day.
Take the first step from home: Send your X-rays and reports to HOSPIDIO for a free, confidential review. Within 24 hours you will know whether reconstruction can help you, what it will cost, and how soon it can be done. Get your free treatment plan here.
Sources
American Academy of Orthopaedic Surgeons (OrthoInfo) - Nonunions
National Institutes of Health / NLM - published reviews on fracture non-union management and the Ilizarov method
HOSPIDIO - ORIF cost in India
Disclaimer: This article is for general information only and does not replace professional medical advice, diagnosis, or treatment. Always consult a qualified orthopedic surgeon regarding your condition.
Recent Blogs



Dr. Basim Parvez is a licensed physiotherapist and Senior Patient Consultant at HOSPIDIO, holding an MBA in Health Management. With extensive clinical experience and a compassionate approach, he assists patients navigating medical treatments. Dr. Basim also leverages his writing talent to simplify complex healthcare information, empowering patients to make informed decisions and fostering clarity and confidence in their medical journeys.
Dr. Hamza Shaikh is a dedicated spine surgeon with over 15 years of experience in spine surgery, specializing in the comprehensive management of spinal deformities such as scoliosis and kyphosis and complex spinal disorders. He currently serves as a Consultant Spine Surgeon at Manipal Hospital, Dwarka, where he provides advanced, evidence-based spine care tailored to both pediatric and adult patients.