If you’re considering knee ligament surgery, you probably have a lot of questions. Whether you’ve just been diagnosed with a torn ACL, MCL, or PCL, or you’re an athlete weighing surgical options, this guide covers everything you need to know. We’ll walk you through how these injuries happen, when surgery is actually necessary, what different surgical approaches look like, and what recovery really entails. If you’re an international patient considering surgery in India, we’ll also cover how to choose a surgeon, plan your travel, and manage your care abroad.
The goal of this guide is to help you make an informed, confident decision about your knee health.
Ready to make an informed decision? Talk to our experienced surgical team.
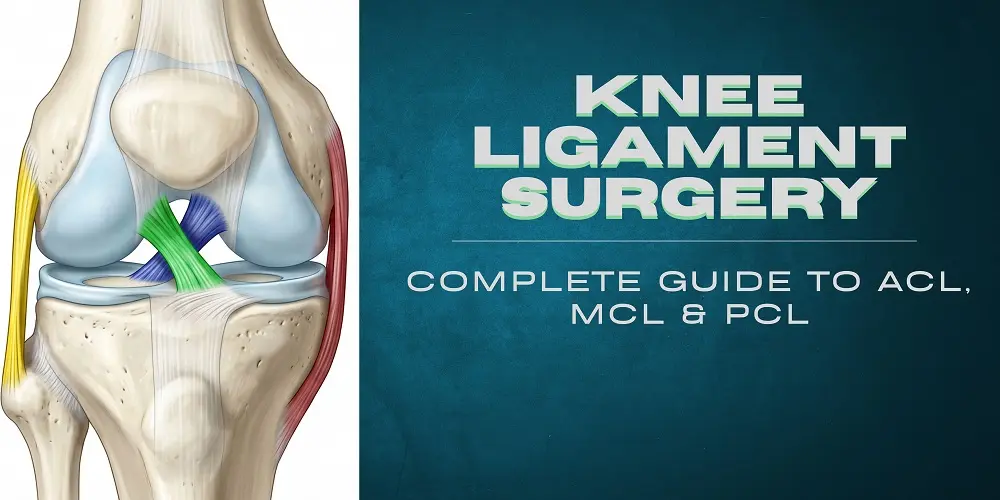
Understanding Your Knee Ligaments: Anatomy & How They Get Injured
Your knee relies on four main ligaments to stay stable and function properly. Each one does a specific job, and when one tears or stretches beyond its limit, it affects how your knee moves and how stable it feels.
The anterior cruciate ligament (ACL) is probably the one you’ve heard about most, especially if you follow sports. It runs diagonally through the middle of your knee and prevents your shin bone from sliding too far forward. That’s why ACL injuries are so common in sports that involve sudden pivoting, cutting movements, or rapid deceleration, think soccer, basketball, skiing, or tennis.
The medial collateral ligament (MCL) runs along the inside of your knee and prevents your knee from bending inward (a movement called valgus stress). Usually, MCL injuries happen from a direct blow to the outside of the knee or from forced inward bending.
The posterior cruciate ligament (PCL) does the opposite of the ACL, it prevents your shin bone from sliding backward. You don’t hear about it as often because it’s less commonly injured, but it’s critical for downhill stability and movements like going down stairs. PCL injuries usually happen from direct blows to the front of the knee (think dashboard injuries in car accidents) or from high-energy trauma.
The lateral collateral ligament (LCL) on the outside of your knee resists outward stress. It’s the least commonly injured of the four, but it’s part of your overall knee stability system.
How Do Knee Ligaments Actually Get Injured?
Ligament injuries happen in different ways depending on the ligament:
- Non-contact pivoting or rapid deceleration , the classic ACL injury scenario. You’re changing direction fast and something doesn’t feel right.
- Direct impact or a blow- MCL and PCL injuries often happen this way. A hit to the side of the knee or a direct trauma can tear these ligaments.
- Hyperextension or severe twisting, when your knee bends too far backward or twists awkwardly.
- High-energy trauma, in accidents or falls, you might injure multiple ligaments at once, which complicates recovery.
Sprain vs. Tear: What’s the Difference?
You might hear the terms “sprain” and “tear” used interchangeably, but there’s actually an important distinction. A sprain means you’ve overstretched or partially torn some of the ligament fibers. There are different grades (I, II, and III), and your ligament can still function, it’s just compromised.
A complete tear (or grade III sprain, depending on how doctors classify it) means the ligament is completely ruptured. This is a more serious injury that usually requires more aggressive treatment, often including surgery. The difference in severity matters because it changes your treatment options significantly.
What Symptoms Should You Watch For?
Knowing what symptoms to look for helps you get diagnosed quickly, especially if you’re booking a remote consultation with a surgeon. Here’s what typically happens when you injure a knee ligament:
Right After the Injury
With an ACL tear, many people report hearing or feeling a “pop”, it’s actually the ligament tearing. You’ll usually feel sudden, sharp pain and your knee will swell rapidly within the first hour or two (this is called hemarthrosis, or bleeding into the joint). You’ll likely feel instability, as if the knee might give way when you try to put weight on it.
Specific Patterns by Ligament
ACL Injuries: That pop you felt, rapid swelling, instability when pivoting, trouble with sudden direction changes.
MCL Injuries: Pain on the inside of your knee, tenderness along the inner joint line, localized swelling on the medial side, pain when the knee is pushed inward.
PCL Injuries: Pain in the back of the knee, difficulty bearing weight initially, instability when going down stairs or walking downhill.
Later Signs You Might Notice
Some symptoms emerge over time. You might experience recurrent episodes of instability, your knee gives way unexpectedly, even with normal activity. Chronic pain, difficulty returning to pivoting sports, or recurrent locking and clicking can indicate not just ligament damage but also meniscal injuries (damage to the cartilage in your knee). These later signs are important when talking to your surgeon because they affect treatment decisions.
How Do Doctors Diagnose Knee Ligament Injuries?
Diagnosis starts with your symptoms and a physical exam. Your surgeon will likely use specific tests that have names you might hear: the Lachman test, anterior drawer test, and pivot-shift test for ACL injuries; valgus stress tests for MCL injuries; and posterior drawer tests for PCL injuries. These tests are surprisingly accurate and tell your surgeon a lot about what’s damaged.
From there, imaging comes into play. X-rays are usually first to rule out fractures and check bone alignment. But the real workhorse for ligament injuries is the MRI (magnetic resonance imaging). MRI is the gold standard because it gives your surgeon a detailed picture of the soft tissues, not just your ligaments, but also your meniscus and cartilage. If you’re sending images to a surgeon abroad, your surgeon will want MRI images.
Sometimes, if diagnosis is still unclear or if there are multiple injuries suspected, your surgeon might perform diagnostic arthroscopy, a minimally invasive procedure where they put a small camera inside your knee to look directly at the damage. This can also double as treatment if surgery is needed.
When Do You Actually Need Knee Ligament Surgery?
Here’s the truth: not every torn ligament needs surgery. The decision depends on several factors working together, and it’s one of the most important conversations you’ll have with your surgeon.
Factors That Influence the Decision
a) Which ligament is damaged and how severely?
Complete tears are more often surgical candidates than partial tears.
b) Do you have functional instability?
This is the big one, if your knee gives way repeatedly, especially during activities you want to do, surgery becomes more likely.
c) What’s your activity level?
Young athletes and very active people typically benefit more from surgery because it lets them return to pivoting and cutting sports.
d) Are there other injuries?
If you have meniscal tears, cartilage damage, or multiple ligament injuries, surgery becomes more likely.
e) Have you tried conservative treatment?
If several months of physical therapy haven’t solved persistent instability, surgery is more likely to be recommended.
What This Means for Each Ligament
ACL: Surgery is commonly recommended if you’re young, active, or want to return to sports. Some older, less active patients can do well without surgery if they modify their activities and do focused rehabilitation. But if you have instability or other injuries alongside the ACL tear, surgery is usually the way to go.
MCL: Many isolated MCL tears heal beautifully with bracing and rehab alone. High-grade complete tears, avulsion injuries (where the ligament pulls away from the bone), or MCL injuries combined with ACL tears are more likely to need surgery.
PCL: Isolated grade I or II PCL injuries often recover well with non-operative care. But if you have chronic PCL insufficiency causing ongoing problems, a high-grade tear, or multiple ligament injuries, reconstruction is usually recommended.
Types of Knee Ligament Surgery: What Are Your Options?
When surgery is indicated, there are several approaches. The specific type depends on which ligament is damaged and the extent of the injury.
ACL Surgery: Reconstruction and Repair
ACL reconstruction is the most common approach. Rather than trying to stitch the torn ligament back together, your surgeon replaces it with a graft. The graft can come from your own body (autograft), typically the hamstring tendon or patellar tendon or from donor tissue (allograft). Many surgeons prefer autografts because they integrate better long-term, though autografts do have a small trade-off: some people experience mild donor-site symptoms like anterior knee pain or temporary hamstring weakness.
The surgery is usually done arthroscopically, meaning your surgeon uses a small camera and minimal incisions. They create tunnels in your bone and secure the graft using screws, buttons, or other fixation devices. Some surgeons perform single-bundle reconstructions (using one graft), while others do double-bundle (two grafts) for specific patient populations. Most commonly, single-bundle is sufficient.
ACL repair simply reattaching or resurfacing your native ligament is possible in select cases, particularly for fresh proximal tears (tears closer to where the ligament attaches to the bone). But repair isn’t the standard for most complete midsubstance tears.
MCL Surgery: Repair, Reconstruction, or Conservative
Because many MCL injuries heal well on their own with bracing and rehabilitation, surgery isn’t always necessary. But if you have a high-grade complete tear that isn’t healing, an avulsion fracture (where the bone pulls away), or an MCL tear combined with other injuries, your surgeon will recommend repair or reconstruction. Often this involves reattaching or reinforcing the ligament using local tissue or a graft.
A common scenario is an ACL injury combined with an MCL injury. Your surgeon might address the ACL surgically while managing the MCL conservatively with bracing and rehabilitation, unless the MCL instability persists.
PCL Surgery: Reconstruction Techniques
PCL reconstruction is more technically demanding than ACL reconstruction because of the anatomical challenges. Like ACL reconstruction, it uses grafts (autograft or allograft) and can be single- or double-bundle. The timing of surgery matters more with PCL injuries doing it too early or too late can affect outcomes. If you have other ligament injuries alongside the PCL tear, your surgeon might stage the procedures or do them simultaneously.
For multi-ligament knee injuries where multiple ligaments are damaged, often from high-energy trauma you need a skilled surgical team. These cases sometimes require staged surgeries and coordinated care between orthopedic, vascular, and plastic surgery specialists.
What Happens During Surgery: The Hospital Experience
Before surgery, your surgical team will want to review your full medical history, do blood work, and ensure any existing medical conditions are optimized. Your anesthesiologist will evaluate you and discuss which type of anesthesia is best for you, usually regional (spinal or epidural), general, or a combination.
On surgery day, you’ll be brought to the operating room and anesthesia will begin. ACL reconstruction typically takes 60 to 90 minutes, though the exact time depends on complexity and whether there are additional procedures like meniscal repair.
Right after surgery, you’ll be in recovery with pain management through regional nerve blocks, oral medications, and other strategies. Your knee will be wrapped in compression bandaging and you’ll be given elevation instructions.
Many arthroscopic ligament procedures are outpatient (same-day discharge) or require just one night in the hospital, depending on regional practice and your specific situation. Your surgeon will give you clear instructions about weight-bearing, bracing, and initial rehabilitation.
Compare your knee surgery options with an experienced surgeon
Recovery After Knee Ligament Surgery: Timeline and Milestones
Recovery is staged and looks different for everyone depending on the procedure, graft type, associated injuries, and how well you adhere to rehabilitation. Here’s what a typical recovery timeline looks like:
Weeks 0-2: Acute Recovery
Main focus: Pain control, wound care, reducing swelling, regaining passive knee extension and starting quadriceps activation.
Weight-bearing: Usually partial weight-bearing or as tolerated with crutches. You’ll likely wear a brace.
What to expect: Pain is normal and manageable. Significant swelling is expected. You’re focused on doing your prescribed exercises even though it feels like a small amount of movement.
Weeks 2-6: Early Rehabilitation
Main focus: Restore range of motion, increase quadriceps strength, progress to full weight-bearing.
Milestones: You should regain full extension (straightening) and reach about 120 degrees of flexion (bending).
What to expect: Pain is decreasing. Swelling is improving. You’re starting closed-chain exercises (where your foot stays in contact with the ground). Many people can walk without crutches by the end of this phase.
Weeks 6-12: Strength Building
Main focus: Build quadriceps and hamstring strength, improve balance and proprioception (your body’s sense of where it is in space).
What to expect: You can walk without pain or swelling. Exercises become more challenging. This is when many people can return to light daily activities.
Months 3-6: Advanced Strengthening
Main focus: Sport-specific drills, progress to plyometrics (jumping and explosive movements), running.
What to expect: You can start low-impact cardio, lift weights, and do movements that prepare your knee for return to sport. Timing varies, some people feel ready earlier, others need more time.
Months 6-12+: Return to Sport
This phase is all about guided return to your sport. Many athletes can return to non-contact sports earlier, but cutting and pivoting sports usually come later. Your surgeon and physiotherapist will likely use objective tests, strength testing, hop tests, movement quality assessments, before clearing you for full return to sport.
The commonly cited 9-12 month timeline for full return to pivoting sports like soccer, basketball, or tennis is based on these testing protocols, not just calendar days. Some athletes return sooner, others need longer.
Recovery Milestones: Typical Timeline for ACL Reconstruction
| Timeline | Main Goals & Milestones |
| Weeks 0-2 | Pain control, wound healing, straight leg raise, regain extension |
| Weeks 2-6 | Full weight-bearing as tolerated, ROM 0-120°, begin closed-chain exercises |
| Weeks 6-12 | Build quadriceps/hamstring strength, balance/proprioception |
| Months 3-4 | Low-impact cardio, progressive resistance training |
| Month 6 | Advanced sport-specific drills, return-to-run tests considered |
| Months 9-12 | Return to pivoting sports if objective tests passed |
| Months 12-18 | Maximal performance for some athletes; ongoing conditioning |
Note: These are average milestones. Specific programs vary, and your surgeon uses objective tests before authorizing return to sport.
Return to Sports: When and How
The question every athlete wants to know is: when can I play again? The answer isn’t just about time, it’s about meeting specific criteria.
The Criteria Your Surgeon Uses
Range of motion: Your knee must bend and straighten as well as your uninjured side.
Strength: Your quadriceps and hamstring muscles must be at least 90% as strong as the uninjured leg (often tested with isokinetic testing).
Neuromuscular control: You need good landing mechanics and balance. Clearance: Your surgeon and physiotherapist both must approve based on objective testing.
Timeline by Sport
Low-impact sports (swimming, cycling): 3-6 months
Running and non-pivoting sports: 4-6 months
Pivoting/cutting sports (soccer, basketball, tennis): 9-12 months or longer
Re-injury is possible, especially if you return too aggressively or skip rehabilitation. Following your rehab protocol and gradually progressing through return-to-play phases reduces this risk significantly.
Outcomes and Success Rates: What to Expect Long-Term
The good news: most people who have knee ligament surgery have positive outcomes. ACL reconstruction has high rates of knee stability and patient satisfaction. Many athletes do return to their sport successfully, though exact return-to-sport rates vary by sport, skill level, and individual factors.
MCL injuries, when managed appropriately, often heal well even without surgery. PCL reconstructions can restore stability, but outcomes depend heavily on timing, technique, and associated injuries.
What influences your outcome? Early appropriate treatment, expert surgical technique, comprehensive rehabilitation, and your adherence to the rehab program all play critical roles. One reality to discuss with your surgeon: there’s a risk of long-term osteoarthritis even after successful reconstruction. This is true even for people who do well short-term.
Success means different things to different people. For some, it’s restoring knee stability and reducing pain. For others, it’s returning to their sport. Have that conversation with your surgeon about what “success” means for your specific situation.
Complications and Risks: What Should You Know?
Every surgery carries risks. Most knee ligament surgeries are routine and go smoothly, but it’s important to discuss potential complications with your surgeon so you know what to watch for.
Pain: Expected in early recovery and managed with pain control strategies and gradual rehabilitation.
Infection: Superficial infections are rare; deep infections are even rarer but require immediate attention.
Graft failure or re-tear: This can happen, particularly with early return to sport or traumatic re-injury. This is why rehabilitation and gradual return-to-play matter so much.
Stiffness: Sometimes scar tissue builds up (arthrofibrosis), causing lost range of motion. Early controlled mobilization prevents this.
Persistent instability: If reconstruction fails or additional pathology is present, instability can persist.
Nerve or blood vesselinjury: Rare with modern arthroscopic techniques. Deep vein thrombosis (DVT): Blood clots can form; your surgeon may recommend prophylaxis, especially for longer flights afterward.
Donor site morbidity: If your surgeon uses a patellar tendon autograft, some people experience anterior knee pain. Hamstring autografts can cause temporary hamstring weakness.
Long-term osteoarthritis: Despite successful reconstruction, there’s a risk of arthritis development years later.
Pain Management After Surgery
Managing pain effectively is crucial for good outcomes because it lets you participate in rehabilitation. Most surgeons use a multimodal approach:
Regional anesthesia: Nerve blocks provide immediate post-op pain relief.
Oral medications: Acetaminophen, NSAIDs like ibuprofen, and short-term opioids if necessary.
Cryotherapy: Ice reduces pain and swelling.
Early controlled movement: Paradoxically, gentle early mobilization reduces pain long-term by preventing stiffness.
When should you be concerned?
If you develop new severe increasing pain, fever, excessive drainage or redness around the incision, contact your surgical team. These could indicate infection or another complication.
Special Considerations for Young Adults and Athletes
Young athletes and high-level competitive players are often candidates for ACL reconstruction. The goal is to restore stability and prevent secondary injuries to the meniscus and cartilage that can happen if you return to pivoting sports with an unstable knee.
Graft choice and surgical timing are tailored to your career goals and, if you’re still growing, your growth plate status. For teenagers and young athletes who are still skeletally immature, surgeons use special growth plate-sparing techniques to avoid damaging the growth plates.
Psychological readiness is also part of recovery for athletes. Returning to sport after injury can create anxiety, and your surgical team often addresses this with counseling and gradual return-to-play protocols.
Non-Surgical Options: When They Work
Not every ligament injury requires surgery. Isolated, low-grade sprains often heal beautifully with conservative management: bracing, activity modification, and physical therapy focused on neuromuscular training to improve strength and proprioception.
This approach works best for low-demand patients (those not returning to pivoting sports), patients with medical contraindications to surgery, or situations where the knee is stable enough with conservative care.
But here’s the key: if conservative care fails meaning you have persistent instability or functional limitations that affect activities you want to do surgery becomes the next step.
Choosing a Surgeon and Hospital in India for Knee Ligament Surgery
If you’re considering surgery in India, there are significant advantages: world-class orthopedic centers with international accreditations (JCI, NABH), surgeons trained in sports medicine and knee reconstruction, and competitive costs. But choosing the right surgeon and hospital matters enormously.
What to Look For
Surgeon qualifications: Look for specialty training in sports medicine or knee reconstruction, not just general orthopedics.
Volume and experience: Surgeons and centers that perform high numbers of ligament reconstructions typically have better outcomes.
Accreditation: JCI or NABH accreditation indicates international standards for safety and quality.
International patient services: Dedicated coordinators, English-speaking staff, and experience with international patients smooth the process.
Facilities: Advanced imaging, modern arthroscopic operating rooms, ICU capability, and comprehensive physiotherapy units.
Track record: Ask for outcomes data, revision rates, infection rates, and typical length of stay.
Steps for International Patients
- Initial remote consultation: Send your clinical history, MRI images (DICOM files ideally), X-rays, and any prior surgical notes for review.
- Get a detailed cost estimate: Include surgeon fees, hospital charges, implants/grafts, anesthesia, medications, physiotherapy, and follow-up visits.
- Plan your travel: The hospital’s international desk usually helps with medical visa documentation.
- Arrange accommodation: Find recovery accommodation close to the hospital. Plan for a caregiver for the first 1-2 weeks.
- Finalize follow-up: Plan for early post-op checks in India and arrange physiotherapy at home. Get detailed discharge and rehabilitation protocols.
Top Orthopedic Surgeons in India for Knee Ligament Surgery






Understanding the Costs
Costs vary widely based on your city, facility type, implant choices, and case complexity. Typical variables include surgeon fees, hospital stay, implants (graft type and fixation devices), imaging, physiotherapy, and medications. You can check the ACL Reconstruction Surgery Cost in India.
Many hospitals offer international packages that bundle consultation, surgery, accommodation, and airport transfer, these give you a clear price upfront. Always ask for an itemized quote so you understand exactly what’s included.
Here’s an important principle: don’t choose solely based on price. Prioritize surgeon expertise and hospital quality. A slightly higher investment in the right surgeon often leads to better outcomes and fewer complications, which saves money long-term.
Travel Preparation Checklist for International Patients
Medical Documents:
- Detailed referral letter from your home physician
- MRI and X-ray images (DICOM files recommended)
- Operative notes if you’ve had prior knee surgery
Personal Documents:
- Medication list and allergy history
- Passport and travel documents
- Travel insurance and medical visa documents
Payment & Logistics:
- Ask about direct billing options
- Arrange payment method
Post-Op Supplies:
- Compression stockings
- Crutches or boots (check if provided)
Rehabilitation:
- Arrange post-op physical therapy with the hospital or partner providers; request detailed rehab protocols to take home.
Considering knee surgery in India? Our team guides international patients through every step. Book a consultation.
Concluding as:
Knee ligament injuries are serious, but modern surgical techniques and rehabilitation protocols have made outcomes predictable and positive for most people. The key is making an informed decision with a skilled surgeon who understands your goals, committing to comprehensive rehabilitation, and being patient with the recovery timeline. Whether you choose surgery at home or travel to India for care, prioritize surgeon expertise and follow your rehab protocol, that’s what determines your long-term success.
Helpful Reads



References
- PMC (PubMed Central) - NIH
- Medscape/eMedicine
- Cleveland Clinic
- Physiopedia
- Journal of Orthopaedic Surgery and Research (Springer)
- UCHealth (University of Colorado)
- Andrews Sports Medicine
- Fowler Kennedy Sport Medicine Clinic
Recent Blogs



FAQs
ACL reconstruction replaces your torn ligament with a graft (from your own tissue or donor tissue). ACL repair reattaches or resurfaces your native ligament and is possible in select proximal tears. Reconstruction is the standard for most complete ACL ruptures because outcomes are more reliable.
Most surgeons advise against long-haul flights for at least 2-6 weeks depending on DVT risk and your comfort level. Discuss air travel timing with your surgeon. They may recommend DVT prophylaxis (blood clot prevention) if you need to fly sooner.
Success depends on how it’s defined. Most studies report good to excellent functional outcomes in the majority of properly selected patients. Many people return to their sport successfully, though re-tear rates and long-term arthritis risk vary by population and study.
Early pain is common but manageable with regional blocks and multimodal analgesia. Most patients describe decreasing pain after the first 1-2 weeks and controllable discomfort during rehabilitation. By 6-8 weeks, pain is usually minimal.
Some patients require revision surgery for graft failure, or to address meniscal or cartilage lesions that become symptomatic. Choosing an experienced surgeon, following rehabilitation, and gradually returning to sport reduces this risk.
Sasmita Bal is a Digital Marketing and Content Specialist at HOSPIDIO with expertise in SEO and international healthcare content. She reviews published material to ensure it is optimized for search visibility and relevant to the needs of international patients seeking treatment in India. All content she reviews is authored and clinically approved by the Founder of HOSPIDIO and relevant medical specialists prior to publication.
Guneet Bhatia is the Founder of HOSPIDIO and an accomplished content reviewer with extensive experience in medical content development, instructional design, and blogging. Passionate about creating impactful content, she excels in ensuring accuracy and clarity in every piece. Guneet enjoys engaging in meaningful conversations with people from diverse ethnic and cultural backgrounds, enriching her perspective. When she's not working, she cherishes quality time with her family, enjoys good music, and loves brainstorming innovative ideas with her team.