If you or a loved one has completed a bone marrow transplant, this guide to bone marrow transplant recovery will help you understand the stages of recovery, the practical care tasks caregivers perform, and the signs that require urgent medical attention. Use this as a day‑by‑day and month‑by‑month companion: read the “first 30 days” section closely if you are still in hospital or recently home, use the checklists and medication templates to organise daily care, review the infection‑prevention and travel sections if you are an international patient planning follow‑up from abroad.
Recovery Phases After a Bone Marrow Transplant
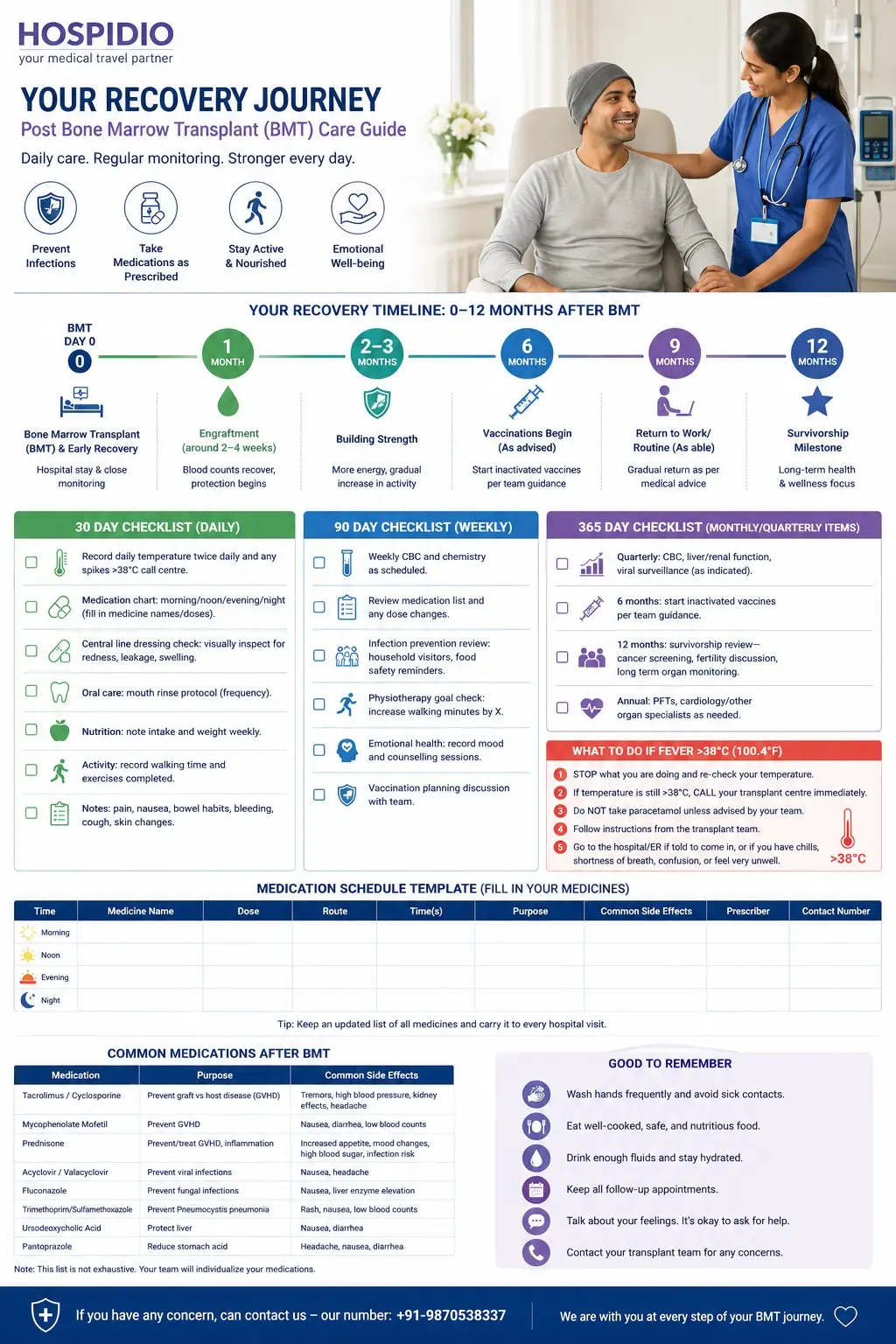
Recovery after a bone marrow transplant generally follows four overlapping phases:
- Immediate (Day 0 - 7): intensive monitoring, isolation/protected environment, and management of immediate complications.
- Early (Weeks 2 - 4): engraftment begins, infection risk still high, transition to outpatient care.
- Intermediate (Months 1 - 3): immune reconstitution accelerates, medications adjusted, beginning rehabilitation and vaccinations planning.
- Long term (Months 3 - 12+): gradual immune recovery, monitoring/management of chronic complications (e.g., chronic GVHD), return to normal activities.
Expect variation: Recovery timelines differ by transplant type (autologous vs allogeneic), underlying disease (leukaemia, lymphoma), age, donor match, conditioning intensity and complications. Below you’ll find practical, evidence‑based steps for each phase, caregiver tasks, medication and nutrition guidance, and downloadable tools.
The First 30 Days in Hospital & Early Home Care
Day 0 - 7: immediate post‑op monitoring and essential care What happens in the first week
- Environment: Most centres keep patients in a single/isolated room with strict infection control (HEPA filters in some units).
- Monitoring: Daily vital signs, daily or more frequent complete blood counts (CBC), fluid and electrolyte checks, and frequent medical reviews.
- Lines & devices: Central venous catheter/port care is critical dressings changed by trained staff, report redness, leakage or pain immediately.
- Symptoms to expect: fatigue, poor appetite, nausea, mouth sores (mucositis), diarrhoea or constipation, mild pain at catheter sites.
- Supportive treatments: IV fluids, pain control, antiemetics, mouth care protocols, transfusions if needed.
- Infection control: Restricted visitors, all visitors and staff must perform hand hygiene. Masks and other PPE may be used depending on centre policy.
- Emotional support: Anxiety and sleep disruption are common ask for counselling, pastoral care or social work support.
Key caregiver actions
- Do not touch central line dressings unless trained. Report any abnormal drainage, swelling, fever, or pain.
- Enforce hand hygiene: soap and water or alcohol rub for all who touch the patient.
- Keep a small, familiar comfort item to reduce stress (subject to unit rules).
- Document all medicines and symptoms in a single notebook for quick handover.
Week 2 - 4: Engraftment Signs, Monitoring and Common Complications, What to Expect
- Engraftment: Neutrophil count recovery (ANC rise) often appears in this window for many patients, platelet counts may lag. Your transplant team will define the lab targets they expect (e.g., ANC > 500/µL on three consecutive days).
- Labs and visits: Frequent outpatient CBCs, renal and liver function tests, and infection surveillance.
- Common complications:
- Mucositis: mouth sores and odynophagia managed with topical rinses, pain control and diet changes.
- Neutropenia and neutropenic fever: any fever >38°C (100.4°F) is an emergency call immediately.
- Viral reactivation (CMV, HSV) or fungal infections in high‑risk patients monitored and sometimes preemptively treated.
- Medications: Prophylactic antibiotics/antifungals/antivirals often continue, immunosuppressants are started or adjusted for allogeneic transplants.
- Mobility: Begin gentle ambulation and breathing exercises, physical therapy may provide a progressive plan.
Caregiver role (practical tips)
- Maintain strict hand hygiene and limit visitors to healthy adults only.
- Prepare safe, approved meals, avoid high‑risk foods (see food safety section).
- Keep a detailed medication log and bring it to every appointment.
- Note and report any changes: new pain, bleeding, cough, rash, headache, changes in urine/stool, or confusion.
Weeks 4 - 12: Immune Rebuilding & Outpatient Care
Clinical priorities during months 1 - 3
- Immune recovery: Lymphocyte counts and functional immunity improve but can remain impaired risk of infection persists.
- Medication management: Doses of immunosuppressants (e.g., ciclosporin, tacrolimus, mycophenolate) are adjusted based on drug levels and clinical status.
- Growth factors: Some patients receive G‑CSF (filgrastim) to stimulate neutrophil recovery early on, typically not continued long term.
- Vaccination planning: Live vaccines are contraindicated, deinstitutionalized vaccination schedules begin later (see months 3–12 section).
- Surveillance: Ongoing CBCs, organ function tests, screening for viral reactivations (CMV, EBV), and chimerism testing in some allogeneic recipients.
- Rehabilitation: Gradual increase in activity levels, structured physiotherapy for deconditioning.
Practical outpatient care tasks
- Medication adherence: Use pill boxes, phone reminders and a medication chart that lists each drug, dose, time and purpose.
- Infection prevention at home: Continue strict hand hygiene, avoid crowds and travel to high‑risk areas in early months.
- Nutrition: Focus on high‑protein, nutrient‑dense foods, manage decreased appetite with small, frequent meals and oral nutritional supplements if advised.
- Follow‑up schedule: Keep all scheduled clinic visits and lab draws these determine when medications can be reduced and when safe milestones are reached.
Months 3 - 12: Late Complications & Long‑term Recovery
Chronic GVHD (graft‑versus‑host disease)
- Who is at risk: Allogeneic transplant recipients only.
- Typical timing: Chronic GVHD often appears after 3 months but can start earlier or much later.
- Common organs involved: Skin, mouth, eyes, GI tract, liver, lungs (bronchiolitis obliterans).
- Symptoms to watch for: New rash, dry eyes/mouth, persistent cough or breathlessness, difficulty swallowing, jaundice.
- Management: Immunosuppressants, topical therapies, physiotherapy (e.g., pulmonary rehab), and multidisciplinary care.
- Long‑term monitoring: Regular pulmonary function tests (PFTs), liver tests, and skin/eye exams as recommended.
Fertility, vaccinations and long‑term organ monitoring
- Fertility: Many conditioning regimens cause temporary or permanent infertility. Discuss fertility preservation before transplant, refer to reproductive specialists as needed.
- Vaccinations: Inactivated vaccines (influenza, pneumococcal conjugate, hepatitis B) are typically restarted starting several months after transplant according to centre protocols, live vaccines are delayed until immune recovery milestones are met.
- Cardiac/renal monitoring: Chemotherapy and conditioning can impact organs, ongoing monitoring may include echocardiography, renal function tests and endocrinology follow‑up.
Return to work, driving & travel (notes for international patients)
- Driving: Avoid driving until your transplant team clears you (varies often several weeks to months, depending on medications and physical recovery).
- Work: Gradual return is common, consider reduced hours and remote work. Immune suppression and infection risk often require workplace accommodations.
- Travel/return home: International patients should plan local follow‑up in India for the early months; arrange clear medical handover and an emergency contact at the treating centre before travel. Some centres offer telemedicine checkups for overseas patients.
Planning long-term follow-up after your transplant? Our international patient team can help with teleconsultation
Infection prevention at home: checklist & best practices Core principles (especially critical in first 3 - 6 months)
- Hand hygiene: Everyone washes hands with soap and water or uses alcohol rub before contact; especially after using the bathroom, handling pets, or preparing food.
- Visitor rules: Only healthy adults should visit; children and anyone with recent respiratory or GI symptoms should not visit.
- Masks: Wear a surgical mask if you have close contact in crowded indoor spaces; some centres recommend masks for visitors during high‑risk periods.
- Food safety:
- Avoid raw/undercooked meats, raw shellfish, sushi with raw fish, unpasteurised milk/cheese and raw sprouts.
- Prefer well‑cooked meats, pasteurised dairy, and thoroughly washed fruits and cooked vegetables.
- Avoid buffets and high‑touch shared food events in early months.
- Household cleaning: Regular cleaning of high‑touch surfaces (doorknobs, remote controls, bathroom fixtures). Avoid dusty renovations and keep humidity controlled to reduce mold.
- Pets: Avoid young animals, reptiles, and animals with diarrhoea. Wash hands after pet contact and avoid litter boxes or cage cleaning if neutropenic.
- When to call: Any fever >38°C (100.4°F), new cough, shortness of breath, vomiting, severe diarrhea, uncontrolled bleeding, sudden confusion or severe pain — contact the transplant centre immediately.
Medication & Symptom Management
Common medications: what they do and what to watch for
- Immunosuppressants (e.g., ciclosporin, tacrolimus, mycophenolate): Prevent GVHD/rejection. Monitor blood levels, kidney function and blood pressure. Common side effects: tremor, hypertension, renal impairment, increased infection risk.
- Antiviral prophylaxis (e.g., acyclovir, valacyclovir): Prevent HSV/VZV reactivation. Report severe headache, rash or neurologic symptoms.
- Antifungal and antibacterial prophylaxis (e.g., posaconazole, fluconazole, trimethoprim‑sulfamethoxazole): Reduce fungal and certain bacterial infections. Watch for gastrointestinal upset, rash or liver enzyme elevations.
- Growth factors (G‑CSF): Stimulate neutrophil recovery. Side effects: bone pain, injection site reactions.
- Pain control and antiemetics: For mucositis and nausea—use as directed; avoid NSAIDs if platelet counts are low unless cleared by team.
Adherence and monitoring tips
- Use a daily medication chart with columns: medicine, dose, time, route, reason, side effects to watch for, and prescriber contact.
- Keep all medications in original packaging for clarity.
- Bring your medication list to every appointment and any other care visits abroad.
- Report new symptoms immediately early recognition reduces morbidity.
Nutrition & Physical Rehabilitation
Nutrition essentials
- Goals: maintain weight, prevent muscle loss, support healing and immune function.
- Protein: Aim for higher protein intake (guided by dietitian, often 1.2-1.5 g/kg/day depending on needs). Use lean meats, eggs, dairy (pasteurised), legumes and high‑protein supplements if needed.
- Calorie intake: Encourage frequent, small meals if appetite is poor; use oral nutrition supplements as recommended.
- Food safety rules (summary): avoid raw/undercooked animal products; ensure fruits/vegetables are washed; avoid unpasteurised products and high‑risk foods like deli salads or buffet items during early months.
Progressive activity plan
- Week 0 - 4: deep breathing exercises, sitting up, short walks in corridor as tolerated; prevent deconditioning and reduce atelectasis risk.
- Months 1 - 3: increase duration and frequency of walks; add gentle strength exercises (resistance bands) as tolerated.
- Months 3 - 12: structured physiotherapy to rebuild muscle mass and stamina; monitor for shortness of breath or chest pain during exercise and stop immediately if these occur.
- Fatigue management: balance activity and rest; prioritise important tasks, use energy‑conserving techniques, and consider graded return to duties at work.
Explore BMT Treatment Options
Psychological and Social Support
Emotional reactions & common challenges
- Normal reactions: anxiety, depression, mood swings, sleep disturbance, fear of relapse, and grief about life changes.
- Caregiver burnout: caregivers often experience exhaustion, guilt and social isolation.
- Practical supports: social work assistance, financial counselling, patient navigators and international patient coordinators.
Support options for international patients
- Tele‑counselling: Many centres provide remote psychological support and counselling for overseas patients.
- Peer support: Online and local support groups (disease‑specific or transplant survivor groups) help share coping strategies.
- Practical tips: Schedule regular short check‑ins with the transplant nurse coordinator; keep a single, accessible summary of your medical history and follow‑up plan for use by local doctors if you return home.
When to Seek Emergency Care - Red Flags
Call your transplant centre or seek emergency care for:
- Fever >38°C (100.4°F) at any time after transplant.
- Sudden or severe shortness of breath, new persistent cough or chest pain.
- Uncontrolled bleeding (nosebleeds that won’t stop, blood in stool/urine), sudden bruising or petechiae.
- New confusion, severe headache, seizures or sudden vision changes.
- Severe abdominal pain, persistent vomiting or inability to tolerate oral intake.
- Sudden severe pain or swelling in a limb (possibility of deep vein thrombosis) or sudden weakness on one side.
If you are overseas and cannot contact your transplant team, seek the nearest emergency department and bring your transplant summary and emergency contact details.
Follow‑up schedule & typical tests (sample timeline)
Note: Actual schedules vary. Use this as a sample to discuss with your transplant team.
Weeks 0 - 4 (inpatient → early outpatient)
Daily -> several times weekly CBCs while inpatient.
Daily vitals, electrolyte panels as needed.
Clinic or telephone check within 24–72 hours after discharge.
Months 1 - 3
Weekly to biweekly CBC, renal and liver function tests.
Viral surveillance tests (CMV PCR) as indicated.
Medication level checks for immunosuppressants (e.g., tacrolimus levels) as directed.
Chest X‑ray or PFTs if respiratory symptoms.
Months 3 - 12
Monthly to every 2 - 3 months: CBC, biochemistry profile, and organ‑specific labs (liver enzymes, kidney tests).
Vaccination schedule begins per centre protocol (inactivated vaccines).
Pulmonary function tests, skin/eye exams and fertility counselling as indicated.
Annual cancer screening and long‑term survivorship planning starting at 1 year.
For International Patients Coming to India, What to Expect
Choosing an accredited BMT centre
Look for centres with JCI or national accreditation, published outcomes, a dedicated international patient office, and multidisciplinary transplant teams.
Ask questions about experience with your diagnosis (e.g., lymphoma, leukemia), type of transplant (autologous/allogeneic), donor selection expertise and availability of follow‑up care.
Practical logistics Handled by HOSPIDIO Team
International patient services: We provide visa invitation letters, dedicated international coordinators, language support, and assistance with accommodation and travel.
Medical records: Provide complete medical records, pathology reports, imaging, blood test results and a transplant summary in English before arrival.
Cost and payment: We will share the treatment plan after your reports are evaluated by our team of specialized doctors. You can check the cost details at Bone Marrow Transplant Cost in India.
Send your reports now for a free evaluation.
Post‑treatment follow‑up: Arrange structured handover for your local physician before travel home and maintain regular telemedicine contact with the Indian centre during the first year
References & Further Reading (Authoritative Resources)
European Society for Blood and Marrow Transplantation (EBMT): https://www.ebmt.org/information-patients-donors
American Society of Hematology (ASH): https://www.hematology.org/
National Comprehensive Cancer Network (NCCN): https://www.nccn.org/patientresources/patient-resources
CDC Guidance: https://www.cdc.gov
WHO Travel Health Guidance: https://www.who.int/publications/i/item/9789241580472
Need expert support for Bone Marrow Transplant recovery or treatment in India?
Recent Blogs



FAQs
The highest infection risk is in the first 3 months, particularly during neutropenia and early vaccination gaps. A fever >38°C (100.4°F) is always urgent.
International travel should be planned with your transplant team; many centres advise staying local for early follow‑up (first 3 months) and completing a formal handover for your local physician before travel.
Many patients return to work part‑time initially and resume full duties over months to a year. Discuss workplace accommodations and timing with your team.
Guneet Bhatia is the Founder of HOSPIDIO and an accomplished content reviewer with extensive experience in medical content development, instructional design, and blogging. Passionate about creating impactful content, she excels in ensuring accuracy and clarity in every piece. Guneet enjoys engaging in meaningful conversations with people from diverse ethnic and cultural backgrounds, enriching her perspective. When she's not working, she cherishes quality time with her family, enjoys good music, and loves brainstorming innovative ideas with her team.
Dr. Akash Khandelwal is a consultant hematologist with clinical expertise in hematologic malignancies, bone marrow transplantation, and advanced cellular therapies, including CAR T-cell therapy. He is actively involved in the management of complex blood cancers and immune disorders, with a strong focus on evidence-based treatment, patient safety, and long-term outcomes. Dr. Khandelwal works closely with multidisciplinary teams to deliver standardized, guideline-driven care for both domestic and international patients, combining clinical precision with a patient-centered approach.